LAST MEDICALLY REVIEWED:
June 2026 — Dr. Shaileshkumar Garge
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad, Telangana 500072
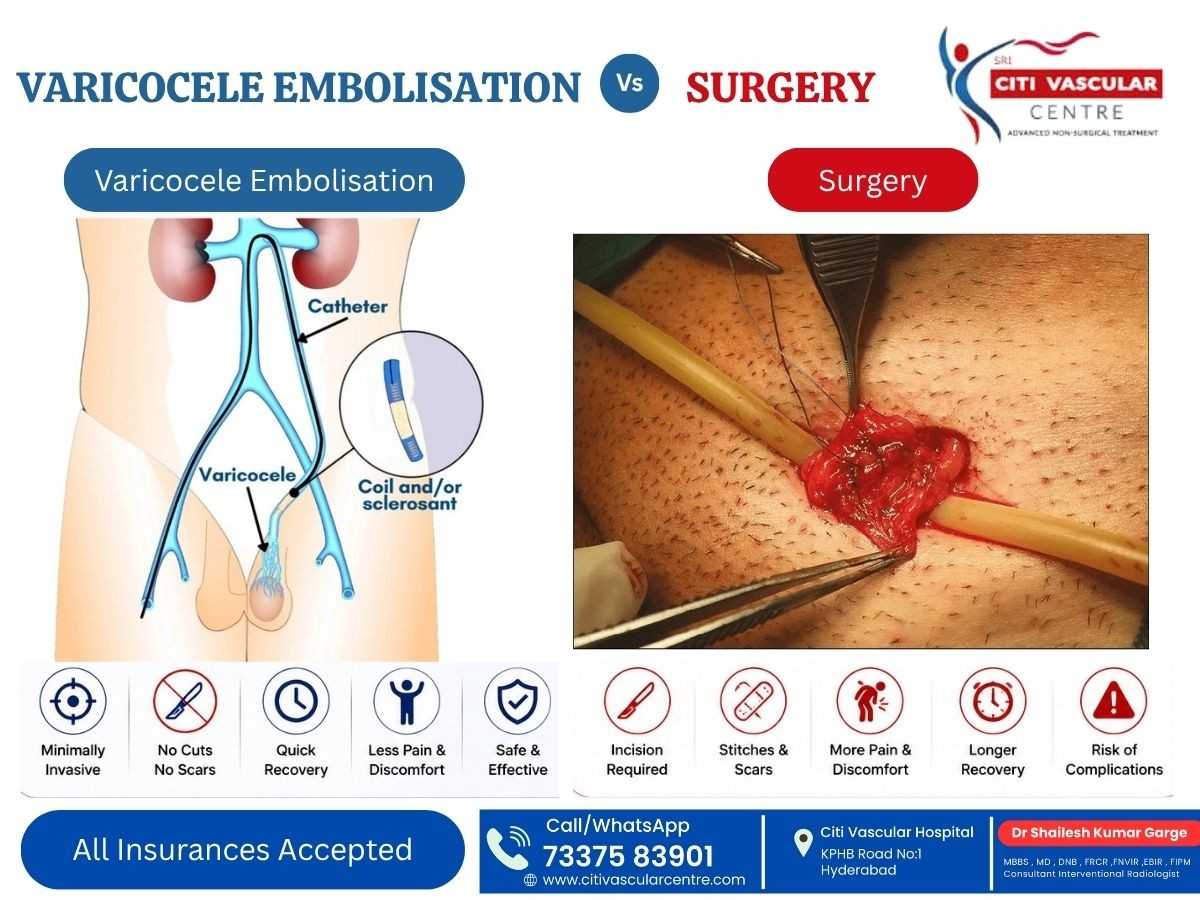
Varicocele surgery and varicocele embolization both effectively treat enlarged scrotal veins — achieving comparable 85–90% symptom success rates. The critical differences lie in HOW they treat it: surgery physically ties the veins through an incision requiring general or spinal anaesthesia and 7–14 days recovery; embolization blocks them from the inside through a 2mm neck or groin puncture using local anaesthesia with same-day discharge and 2–3 day recovery.
The choice between surgery and embolization is not about which works — both do. It is about which approach best fits your symptoms, fertility goals, anatomy, prior treatment history, and recovery needs. For many suitable patients, embolization offers faster recovery, no surgical incision, minimal scarring, and same-day discharge.
This complete comparison guide by Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain) — at Citi Vascular Hospital, KPHB, Hyderabad covers every dimension of this decision: procedure mechanics, recovery, fertility outcomes, risks, success rates, costs, and which patients are best suited to each approach — so you can walk into your consultation fully informed.
QUICK ANSWER
Varicocele Surgery vs Embolization — The Short Answer
Both achieve 85–90% symptom success. Embolization: no incision, local anaesthesia, 2–3 day recovery, same-day discharge, < 1% hydrocele risk. Surgery: slightly lower recurrence with microsurgery, but general / spinal anaesthesia, 7–14 day recovery, 5–15% hydrocele risk.
Book a Varicocele Consultation — Surgery vs Embolization Assessed Together
Dr. Shaileshkumar Garge FRCR (UK) | Citi Vascular Hospital, KPHB, Hyderabad | All treatment options available
+91-73375 83901 | WhatsApp | citivascularcentre.com
|
Feature |
Varicocele Embolization |
Varicocele Surgery (Best: Microsurgery) |
|
Treatment Type |
Minimally invasive — image-guided |
Surgical — open or laparoscopic or micro |
|
Surgical Incision |
❌ No — 2mm puncture only |
✅ Yes — inguinal, abdominal, or scrotal |
|
Stitches |
❌ No |
✅ Yes — skin closure required |
|
Anaesthesia |
Local +/- sedation only |
General or spinal anaesthesia |
|
Procedure Duration |
15–45 min (unilateral); 30-60 min (bilateral) |
60–90 min (microsurgery) |
|
Hospital Stay |
Same-day discharge |
1–2 days |
|
Return to Work |
2–3 days (desk); 5–7 days (physical) |
7–14 days |
|
Hydrocele Risk |
< 1% |
~2–10% (varies by technique) |
|
Recurrence Rate |
~5–10% at 2 years |
~1–5% (microsurgery — lowest of all) |
|
Bilateral Treatment |
✅ Both sides in ONE session |
Usually 2 separate operations |
|
Success Rate (symptom relief) |
85–90% |
75–90% (varies by technique) |
|
Recurrent Post-Surgery Varicocele |
✅ Preferred — avoids scarred tissue |
⚠️ Technically difficult — repeat dissection |
|
Cost Hyderabad 2026 |
₹60,000–₹1,40,000 |
₹70,000–₹1,50,000 (microsurgery) |
|
Performed By |
Interventional Radiologist exclusively |
Urologist or General Surgeon |
Bottom Line: Both treatments work. Embolization wins on recovery, convenience, bilateral treatment, and hydrocele risk. Microsurgery wins on the lowest long-term recurrence rate. The right choice depends on your specific clinical situation — discussed in detail in Section 9.
Varicocele is the abnormal enlargement of the pampiniform plexus — a network of small veins that drain blood from the testicles back into the systemic circulation. When the valves in the internal spermatic vein become incompetent, blood pools and flows backwards (reflux) into the scrotal veins, causing them to dilate.
|
Key Fact |
Detail |
|
Prevalence |
15% of all men; up to 40% of men investigated for male infertility |
|
Most Common Side |
Left side (~90%) — due to left renal vein anatomy; bilateral in ~30–40% |
|
Why It Causes Problems |
Backflow raises scrotal temperature 1–2°C above optimal — impairs spermatogenesis; venous congestion causes pain |
|
When Treatment Is Needed |
Persistent pain | Abnormal semen parameters | Testicular atrophy | Symptoms affecting quality of life |
|
Treatment Options |
Observation | Embolization | Microsurgical varicocelectomy | Laparoscopic varicocelectomy | Open surgery |
How Varicocele Surgery Works
Varicocelectomy (varicocele surgery) physically identifies, isolates, and ties off / clips / divides the abnormal internal spermatic vein and its branches through a surgical incision. Blood flow is permanently redirected to healthy venous collaterals. All surgical approaches require anaesthesia, an incision, and a recovery period.
Types of Varicocele Surgery
|
Approach |
Incision Location |
Anaesthesia |
Key Advantage |
Recurrence Risk |
|
Open / Retroperitoneal |
Flank or low abdominal |
General/Spinal |
Straightforward access |
Higher (~15%) |
|
Inguinal (Palomo) |
Groin crease |
General/Spinal |
Widely performed technique |
~10–15% |
|
Subinguinal Microsurgery |
Below groin crease |
General/Spinal |
Lowest recurrence + lowest hydrocele risk of all surgical approaches |
~1–5% (best) |
|
Laparoscopic |
3 small abdominal ports |
General |
Bilateral in one session possible |
~3–7% |
Surgical Procedure — Stage by Stage
|
Step |
Stage |
What Happens |
|
1 |
Anaesthesia |
General or spinal anaesthesia administered in the operating theatre — patient asleep or lower half numb |
|
2 |
Surgical Incision |
Incision made at the inguinal ligament (groin), retroperitoneal (flank), or subinguinal region — 3–5 cm typically |
|
3 |
Vein Identification |
Internal spermatic vein and its branches are identified under direct vision — microsurgery uses operating microscope for magnification |
|
4 |
Arterial Preservation |
Testicular artery, lymphatic vessels, and vas deferens are carefully preserved using magnification (microsurgery) or Doppler probe |
|
5 |
Vein Ligation / Division |
All abnormal venous channels are tied off and divided. Clips or sutures are applied to prevent blood flow |
|
6 |
Wound Closure |
Surgical incision is closed with sutures or staples in layers. Dressing applied. Takes 60–90 minutes total |
|
7 |
Hospital Stay + Recovery |
1–2 days in hospital. Return to desk work: 7–10 days. Physical activity: 2–4 weeks. Follow-up at 3–6 months |
How Varicocele Embolization Works
Varicocele embolization blocks the abnormal internal spermatic vein FROM INSIDE the blood vessel — without any surgical incision. A 2mm catheter advanced through the neck or groin vein under real-time X-ray (fluoroscopy) deposits embolic agents precisely within the abnormal vein, permanently sealing it. Blood reroutes to healthy collateral veins naturally.
Embolization Techniques — Which Is Used When?
|
Technique |
Embolic Material |
Mechanism |
Best Used For |
|
Coil Embolization |
Platinum / stainless steel coils |
Mechanical plug — coils expand to fill and block vein lumen permanently |
Primary embolization of main internal spermatic vein — most common first-line technique |
|
Sclerosant Embolization |
Polidocanol / Sodium Tetradecyl Sulfate (STS) foam |
Chemical sclerosant injected — causes vein wall inflammation and permanent closure |
Small collateral branches unreachable by coils; combined with coils for complete occlusion |
|
Combined Technique |
Coils + sclerosant foam |
Coils block main vessel; sclerosant treats residual branches and collaterals |
Bilateral cases | infertility optimisation | complex anatomy — lowest recurrence rate of all embolization techniques |
|
Liquid Embolic Agents |
Onyx / NBCA polymer |
Viscous polymer solidifies on contact with blood — fills tortuous venous anatomy |
Complex recurrent varicocele where anatomy is unpredictable post-prior surgery |
Embolization Procedure — Stage by Stage
|
Step |
Stage |
What Happens |
|
1 |
Local Anaesthesia |
Brief sting at neck or groin — area fully numb within 60 seconds. You remain awake and comfortable throughout. |
|
2 |
Catheter Insertion |
2mm sheath inserted through neck (jugular) or groin (femoral) vein via tiny puncture. No incision, no stitches. |
|
3 |
Navigation Under Fluoroscopy |
Guide wire and catheter advanced under live X-ray to the left internal spermatic vein (and right if bilateral) |
|
4 |
Venography — Roadmap |
Contrast dye maps the entire abnormal venous network — identifies all branches, collaterals, and reflux points to be treated |
|
5 |
Embolization |
Coils / foam / liquid embolic deployed precisely into abnormal veins. Complete blockade confirmed under fluoroscopy. |
|
6 |
Bilateral (If Needed) |
Catheter repositioned to right gonadal vein — same steps repeated. BOTH SIDES in ONE session. |
|
7 |
Final Verification + Discharge |
Post-embolization venography confirms complete occlusion. Catheter removed. neckband or brief pressure applied. Home same day. |
|
Feature |
Embolization |
Microsurgery |
Laparoscopic |
Open Surgery |
|
Incision |
❌ None |
✅ Subinguinal |
✅ 3 ports |
✅ Groin/Flank |
|
Stitches |
❌ No |
✅ Yes |
✅ Yes |
✅ Yes |
|
Anaesthesia |
Local only |
General/Spinal |
General |
General/Spinal |
|
Duration |
15-60 min |
60–90 min |
45–75 min |
45–60 min |
|
Hospital Stay |
Same day |
1–2 days |
1–2 days |
1 day |
|
Return to Work |
2–3 days |
7–14 days |
7–10 days |
7–14 days |
|
Hydrocele Risk |
< 1% |
~2–5% |
~5–10% |
~10–15% |
|
Testicular Artery Injury Risk |
Nil — no surgical dissection |
< 1% with microscope |
~1–3% |
~3–5% |
|
Recurrence Rate |
~5–10% |
~1–5% |
~3–7% |
~10–15% |
|
Bilateral — Same Session? |
✅ Yes — always |
Needs 2 operations |
Usually yes |
Needs 2 operations |
|
Success Rate (symptoms) |
85–90% |
75–90% |
70–85% |
70–80% |
|
Recurrent Post-Surgery? |
✅ Preferred — no re-dissection |
⚠️ Difficult — scarring |
Possible |
⚠️ Difficult |
|
Fertility Improvement |
60–70% of cases |
60–70% of cases |
55–65% |
50–65% |
|
Semen Analysis at 3–6 months |
Required for all |
Required for all |
Required |
Required |
|
Cost Hyderabad 2026 |
₹60K–₹1.4L |
₹70K–₹1.5L |
₹80K–₹1.5L |
₹40K–₹80K |
|
Recovery Stage |
Embolization |
Surgery (Microsurgery) |
|
Day 0 — Procedure Day |
Mild pelvic ache. Discharged same afternoon. |
Awake from general anaesthesia | Monitored overnight in hospital |
|
Days 1–2 |
Home rest. Light activity. 80% of men feel near-normal. |
Hospital stay | Wound care | Catheter if used | Pain managed with IV then oral meds |
|
Days 2–3 |
Return to desk work. Drive after Day 2. |
Discharge from hospital. Wound care at home. Sutures in situ. |
|
Day 7 |
Full normal activity. Exercise from Day 7. |
Suture removal visit. Office work beginning for most patients. |
|
Days 7–14 |
No restrictions. light gym/cycling from Day 10. |
Return to work for most. No heavy exercise yet. |
|
Weeks 3–4 |
Normal — follow-up Doppler booked at 3 months. |
Return to physical work and exercise for most. Wound fully healed. |
|
Month 3 |
Follow-up Doppler confirms successful occlusion. |
Follow-up Doppler confirms surgical outcome. |
|
Month 3–6 |
Semen analysis if infertility was indication. |
Semen analysis if infertility was indication. |
Recovery Warning Signs — Contact Citi Vascular Immediately: Fever > 38.5°C | Increasing (not decreasing) pain after Day 3 | Worsening swelling at access site or surgical wound | Discharge or oozing that soaks dressings | Feeling systemically unwell. Call +91-73375 83901.
Success Rate Comparison
|
Outcome |
Embolization |
Microsurgery |
|
Technical success (vein occlusion confirmed) |
95–98% |
98–99% |
|
Overall symptom relief |
85–90% |
75–90% |
|
Scrotal pain resolution |
75–90% at 3 months |
70–85% at 3 months |
|
Semen parameter improvement |
60–70% of infertility cases |
60–70% of infertility cases |
|
Spontaneous pregnancy rate post-treatment |
~30–45% |
~35–50% |
|
Hydrocele formation |
< 1% |
~2–5% (microsurgery) |
|
Varicocele recurrence at 2 years |
~5–10% |
~1–5% (lowest of all) |
|
Patient satisfaction |
85–95% |
80–90% |
Fertility Note: Both treatments show comparable semen parameter improvement (~60–70%) and spontaneous pregnancy rates (~30–50%). The slight edge in pregnancy rates seen with microsurgery in some studies may relate to better patient selection and lower hydrocele complication rates rather than the surgical approach itself. Results are highly individual.
Risk Comparison — What Could Go Wrong?
|
Risk |
Embolization |
Surgery (Microsurgery) |
|
Hydrocele (fluid collection) |
< 1% — very rare |
~2–5% (microsurgery) — 10–15% (open surgery) |
|
Wound infection |
Not applicable — no incision |
~2–4% — treated with antibiotics |
|
Bleeding / haematoma |
Minimal — 2mm puncture |
~1–3% — wound haematoma possible |
|
Testicular artery injury |
Zero — no surgical dissection |
< 1% with microscope; higher with open technique |
|
Testicular atrophy (post-op) |
Not reported — no arterial risk |
Rare (< 0.5%) — if testicular artery compromised |
|
Anaesthesia risk |
Minimal — local only |
General/spinal anaesthesia risk: ~1–3% mild adverse events |
|
Coil migration |
< 0.5% — expert technique prevents |
Not applicable |
|
Contrast reaction |
< 0.5% — pre-screened and managed |
Not applicable |
|
Recurrence |
~5–10% — re-embolization possible |
~1–5% microsurgery — lowest of all techniques |
Note: Embolisation is safer than surgery.
9. WHICH TREATMENT IS BETTER? — DECISION GUIDE
Choose Embolization When:
|
Clinical Situation |
Why Embolization Is Preferred |
|
Bilateral varicocele (both sides) |
Both treated in ONE session — surgery would require two separate operations with two recoveries |
|
Recurrent varicocele after prior surgery |
Avoids re-dissection of scarred tissue — approaches the vein from the neck/groin, bypassing the prior surgical site entirely |
|
Wishes to avoid general anaesthesia |
Local anaesthesia only — no anaesthetic risk, no intubation, no post-anaesthesia nausea |
|
Cannot take time off work (>3 days) |
Back to desk work in 2–3 days vs 7–14 days after surgery — most economically practical option |
|
Concerns about surgical scarring |
2mm neck or groin puncture — virtually invisible within 2 weeks. No abdominal or groin scar. |
|
Prefers minimally invasive treatment |
No general anaesthesia | no hospital stay | same-day discharge — full procedure 30–60 minutes |
|
IVF / ICSI planning within 6 months |
Embolization 3–6 months before IVF cycle can improve sperm quality — same timeline and outcomes as surgery |
Consider Microsurgery When:
|
Clinical Situation |
Why Microsurgery May Be Preferred |
|
Lowest possible recurrence rate is the priority |
Microsurgery achieves ~1–5% recurrence vs ~5–10% for embolization — if recurrence would be catastrophic (e.g. high-stakes IVF), this matters |
|
Unusual venous anatomy making embolization difficult |
Rare anatomical variants (retroaortic renal vein, dual spermatic veins) may make catheter access to the spermatic vein technically challenging |
|
Patient strongly prefers a surgical approach |
Some patients prefer the 'definiteness' of physical vein ligation. Both approaches are valid when the patient is fully informed. |
|
Concurrent inguinal hernia or hydrocele repair needed |
If hernia or hydrocele repair is also planned, combining with microsurgical varicocelectomy in a single general anaesthetic may be practical |
'Which Treatment Is Right for Me?' — Decision Flowchart
|
Step |
Check This Question |
YES → Direction |
NO → Direction |
|
1 |
Do you have bilateral varicocele (both sides confirmed on Doppler)? |
→ Embolization strongly preferred — single session bilateral treatment |
→ Step 2 |
|
2 |
Have you had previous varicocele surgery with recurrence? |
→ Embolization strongly preferred — avoids re-dissection |
→ Step 3 |
|
3 |
Can you afford 7–14 days off work for recovery? |
→ Both options open — discuss anatomy at consultation |
→ Embolization: only 2–3 days off work |
|
4 |
Is the lowest possible recurrence rate your #1 priority (e.g., high-stakes IVF)? |
→ Microsurgery may offer marginal edge at ~1–5% vs embolization ~5–10% |
→ Embolization remains a strong option — discuss |
|
5 |
Do you wish to avoid general anaesthesia? |
→ Embolization — local anaesthesia only |
→ Both options applicable |
|
6 |
Is embolization technically feasible based on your Doppler/venogram anatomy? |
✅ Proceed with embolization at Citi Vascular KPHB |
→ Microsurgery is the recommended surgical option |
IMPORTANT: There is no single 'better' treatment for all patients. Both are established, evidence-based options. The decision is always made INDIVIDUALLY at consultation after reviewing Doppler imaging, semen analysis, symptom history, anatomy, prior treatments, and patient preferences.
|
Cost Factor |
Embolization |
Microsurgery |
Open Surgery |
|
Procedure Cost |
₹60K–₹1.4L |
₹70K–₹1.5L |
₹40K–₹80K |
|
Anaesthesia |
Included in procedure |
General — adds ₹5K–₹15K |
General — adds ₹5K–₹15K |
|
Hospital Stay |
Day-care — minimal stay cost |
1–2 nights — ₹5K–₹20K/night |
1 night typically |
|
Days Off Work (at ₹1K/day) |
₹2K–₹3K (2–3 days) |
₹7K–₹14K (7–14 days) |
₹7K–₹14K |
|
Hydrocele Treatment If Occurs |
< 1% risk — minimal cost impact |
~5% risk — potential additional ₹20K–₹40K |
~10% risk — potential additional cost |
|
Estimated Total Economic Cost |
₹65K–₹1.45L |
₹85K–₹1.85L |
₹50K–₹1.1L |
→ For a complete cost breakdown with component pricing, insurance coverage details, and EMI amounts: citivascularcentre.com/varicocele-treatment-cost-in-hyderabad
|
Patient Profile |
Clinical Situation |
Recommended Treatment |
Key Reason |
|
Ravi, 29, IT Engineer |
Left varicocele | pain | normal semen | first treatment |
Embolization |
Faster recovery | minimal time off work | local anaesthesia only |
|
Suresh, 34, Married, Infertility |
Left varicocele | low sperm count | planning IVF in 6 months |
Either — discuss timing |
Both achieve comparable fertility outcomes; embolization recovery faster before IVF cycle |
|
Anil, 38, Recurrent Varicocele |
Left recurrence after prior surgery 3 years ago |
Embolization strongly preferred |
Avoids re-dissection of post-surgical scarring — embolization bypasses prior site entirely |
|
Kiran, 32, Bilateral Varicocele |
Both left and right confirmed on Doppler | pain both sides | normal semen |
Embolization |
Both sides treated in one 45–60 minute session — surgery would need two separate operations |
|
Prasad, 36, High-Stakes IVF |
Severe oligospermia | last attempt IVF | wants lowest possible recurrence |
Microsurgery consideration |
Marginally lower recurrence (~1–5%) may matter in high-stakes fertility context — discuss individually |
|
Venkat, 41, Cannot Take Time Off |
Left varicocele | pain | working father | only 3 days available |
Embolization |
Back to desk work in 2–3 days — microsurgery would require 7–14 days off work |
|
Credential |
Detail |
|
Full Name |
Dr. Shaileshkumar Garge |
|
Qualifications |
MBBS | MD (Mumbai) | DNB (Delhi) | FRCR (UK) | FNVIR (CMC Vellore) | EBIR (Spain/Europe) | Fellowship (North Carolina, USA) |
|
Role |
Director & Chief Vascular Physician | Senior Consultant Interventional Radiologist |
|
Hospital |
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad, Telangana 500072 |
|
Varicocele Expertise |
Non-surgical varicocele embolization | bilateral same-session treatment | recurrent post-surgical varicocele embolization |
|
Philosophy |
"Embolization and microsurgery both have their place. My job at consultation is to determine which suits each individual patient — not to default to one approach for all." |
|
Experience |
12+ years | 15,000+ minimally invasive procedures | All varicocele embolization techniques available |
Q1: Is varicocele embolization better than surgery?
For most patients, embolization offers significant practical advantages: no incision, local anaesthesia, same-day discharge, 2–3 day recovery (vs 7–14 days for surgery), < 1% hydrocele risk (vs 2–15% for surgery), and bilateral treatment in ONE session. Microsurgery has marginally lower recurrence (~1–5% vs ~5–10%). Both achieve 85–90% symptom success. The best choice depends on anatomy, bilateral disease, prior surgery history, and individual circumstances.
Q2: Which varicocele treatment has faster recovery?
Varicocele embolization has significantly faster recovery. Most men return to desk work within 2–3 days after embolization — compared to 7–14 days after microsurgery or open surgery. Same-day discharge is standard for embolization vs 1–2 nights in hospital for surgery. Full activity including gym and cycling typically resumes by Day 7–10 after embolization vs 3–4 weeks after open surgery.
Q3: Which treatment is better for male infertility — surgery or embolization?
Both varicocele embolization and microsurgery achieve comparable fertility outcomes — approximately 60–70% semen parameter improvement and 30–50% spontaneous pregnancy rates in appropriately selected patients. Semen improvement takes 3–6 months with both approaches. Some studies suggest microsurgery has marginally higher pregnancy rates, possibly due to lower hydrocele complication risk. Individual factors including female fertility and baseline semen quality are equally important.
Q4: Does varicocele surgery cause hydrocele?
Yes — hydrocele (fluid collection around the testicle) is the most significant complication of varicocele surgery. Risk varies by technique: microsurgery ~2–5%, laparoscopic ~5–10%, open surgery ~10–15%. Hydrocele occurs when the lymphatic vessels are accidentally tied during vein ligation. Varicocele embolization has a hydrocele risk of less than 1% — a major advantage over surgical approaches.
Q5: Can varicocele embolization treat recurrent varicocele after surgery?
Yes — and embolization is the PREFERRED option for recurrent varicocele following prior surgery. Repeat varicocele surgery requires dissecting through scar tissue from the previous operation, which is technically demanding and carries higher complication risk. Embolization approaches the abnormal spermatic vein from the neck or groin via a completely fresh pathway, entirely bypassing the previously operated area. Dr. Garge at Citi Vascular KPHB specialises in this.
Q6: What is the recurrence rate of varicocele after embolization vs surgery?
Varicocele recurrence rates at 2 years: embolization ~5–10% | microsurgery ~1–5% (lowest of all approaches) | laparoscopic ~3–7% | open surgery ~10–15%. Microsurgery has the lowest recurrence because the surgical magnification identifies and ties even the smallest venous branches. Embolization recurrence can be re-treated with repeat embolization. Both options have acceptable recurrence rates for most patients.
Q7: Is general anaesthesia required for varicocele surgery?
Yes. All forms of varicocele surgery (microsurgery, laparoscopic, open) require general or spinal anaesthesia — meaning you are unconscious or partially numb below the waist. Varicocele embolization uses only local anaesthesia and rarely conscious sedation — you remain awake and comfortable throughout without any general anaesthetic. This is a significant advantage for men with anaesthesia concerns, respiratory conditions, or those wishing to avoid general anaesthesia.
Q8: Which is more expensive — surgery or embolization?
Procedure costs are comparable: embolization ₹60,000–₹1,40,000 vs microsurgery ₹70,000–₹1,50,000 in Hyderabad 2026. However, total economic cost often favours embolization: same-day discharge (no hospital stay cost), 2–3 days off work (vs 7–14 days), and < 1% hydrocele risk (vs 2–15%). For bilateral varicocele, embolization treats both sides in one session — surgery requires two separate procedures and recoveries.
Q9: Can bilateral varicocele be treated in one surgical session?
Varicocele embolization treats bilateral (left and right) varicocele in a single 30-60 minute session through one access point. Most surgical techniques require two separate operations — usually staged weeks apart — for bilateral varicocele. Laparoscopic varicocelectomy can treat both sides in one general anaesthetic session, but still carries general anaesthesia risk and longer recovery. Embolization's bilateral single-session approach is one of its strongest practical advantages.
Q10: What are the risks specific to varicocele embolization?
Specific risks of varicocele embolization include: coil migration to the pulmonary vasculature (< 0.5% — prevented by correct coil sizing), pelvic vein irritation/phlebitis (~3–5% — self-resolving with NSAIDs), post-embolization syndrome (mild fever, ache — ~10–20%, resolves in 2–4 days), contrast allergy (< 0.5% — pre-screened), and varicocele recurrence (~5–10%). Hydrocele and testicular artery injury do not occur as no surgical dissection is performed.
Q11: How long does semen improvement take after varicocele treatment?
Semen parameter improvement takes 3–6 months after both embolization and surgery — because the human spermatogenesis cycle takes ~74 days. The first measurable improvement appears at the 3-month semen analysis. Maximum benefit is assessed at 6 months. Do not expect immediate fertility improvement. A semen analysis at both 3 months and 6 months post-treatment tracks the improvement. Most fertility benefit, if it occurs, is seen by 6 months.
Q12: Who performs varicocele embolization in Hyderabad?
Varicocele embolization is performed by Interventional Radiologists — not urologists or general surgeons. At Citi Vascular Hospital, KPHB, Hyderabad, Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain), Fellowship (USA) — performs both bilateral and recurrent varicocele embolization using a dedicated Cath Lab with real-time fluoroscopy. 12+ years experience, 15,000+ minimally invasive procedures. Call +91-73375 83901 for a consultation.
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad — both varicocele embolization and referral coordination for surgical options available for patients from:
Kukatpally & KPHB — 5 min drive
Miyapur & Bachupally — 10 min
Hitech City & Madhapur — 20 min
Ameerpet — 20 min
Gachibowli & Kondapur — 25 min
Secunderabad — 25 min
Kompally, Medchal & Alwal — 20–25 min
Telangana & AP — outstation consultations available
|
Hospital |
Contact |
Location & Hours |
|
Citi Vascular Hospital |
+91-73375 83901 |
KPHB Colony, Road No. 1, Hyderabad, Telangana 500072 | Mon–Sat 9AM–6PM |
|
Booking |
citivascularcentre.com |
WhatsApp + online + walk-in | Same-day consultation available |
|
✅ |
Both embolization and microsurgery achieve 85–90% overall symptom success — the choice is about HOW, not IF, treatment works |
|
✅ |
Embolization: no incision, local anaesthesia, same-day discharge, 2–3 day recovery, < 1% hydrocele risk, bilateral in one session |
|
✅ |
Microsurgery: marginally lowest recurrence rate (~1–5%), possible slight pregnancy rate advantage — but general anaesthesia, 7–14 day recovery |
|
✅ |
Embolization is the PREFERRED treatment for: bilateral varicocele, recurrent post-surgical varicocele, and men who cannot afford 7–14 days off work |
|
✅ |
Both treatments require semen analysis at 3 and 6 months — fertility improvement takes 3–6 months for both approaches |
|
✅ |
The treatment decision should be individualised — assessed with Doppler imaging, semen analysis, and a consultation with Dr. Garge at Citi Vascular KPHB |
Varicocele surgery and varicocele embolization are both evidence-based, highly effective treatments for enlarged scrotal veins. Surgery physically ties the abnormal veins through an incision requiring general anaesthesia and 7–14 days recovery. Embolization blocks them from the inside through a 2mm neck or groin puncture using local anaesthesia — with same-day discharge and 2–3 day recovery.
For most patients today, embolization offers decisive practical advantages: no incision, no stitches, no general anaesthesia, same-day discharge, 2–3 day return to work, bilateral treatment in one session, and < 1% hydrocele risk. Microsurgery retains a specific advantage in the lowest long-term recurrence rate (~1–5%) — relevant when minimising the chance of needing retreatment is the absolute priority.
The best treatment is not determined by a single universal recommendation — it is determined by YOUR anatomy, symptoms, fertility goals, bilateral involvement, prior surgery history, and recovery needs. Dr. Shaileshkumar Garge at Citi Vascular Hospital, KPHB, Hyderabad reviews all of these factors at your consultation and recommends the most suitable approach for your specific situation.
Book Your Varicocele Consultation — Surgery + Embolization Both Assessed
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad
Dr. Shaileshkumar Garge | FRCR (UK) | FNVIR (CMC Vellore) | EBIR (Spain) | 12+ Years | 15,000+ Procedures
+91-73375 83901 | WhatsApp Now | citivascularcentre.com
Same-Day Discharge | Insurance Assisted | EMI Available | All Options Discussed Openly | Mon–Sat 9AM–6PM