LAST MEDICALLY REVIEWED:
June 2026 — Dr. Shaileshkumar Garge
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad, Telangana 500072
Introduction + Quick Answer
Quick Facts Table
What Is Varicocele Embolization?
How Varicocele Forms + Why Embolization Works
Who Should Consider Embolization?
Types, Techniques & Embolic Materials
Pre-Procedure Checklist
Step-by-Step Embolization Procedure (8 Steps)
Recovery Timeline After Varicocele Embolization
Success Rates & Clinical Outcomes
Risks, Complications & Warning Signs
Varicocele Embolization & Male Fertility
Embolization vs Surgery — Full Comparison
Cost Overview (link to cost guide)
Patient Journey — Step-by-Step Story
Doctor Credentials — E-E-A-T Block
FAQ — 10 Q&As at 40–60 Words
Varicocele Embolization Near You in Hyderabad
Key Takeaways
Summary + CTA
Varicocele embolization in Hyderabad is a minimally invasive, image-guided procedure that treats varicocele — enlarged scrotal veins — without any surgical incision, general anaesthesia, or overnight hospital admission. A 2mm catheter inserted through the groin or neck permanently blocks the abnormal veins, achieving 85–90% clinical success with return to routine activities in 1-2 days.
Performed by Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain) — at Citi Vascular Hospital, Kukatpally Colony, Hyderabad, varicocele embolization is available for men with scrotal pain, abnormal semen parameters, testicular atrophy, or recurrent varicocele after prior surgery. Patients from Kukatpally, Miyapur, Hitech City, Ameerpet, Secunderabad, and across Telangana are treated here.
This complete guide covers: what varicocele embolization is, how it works, the step-by-step procedure in clinical detail, all embolic techniques and materials, full pre- and post-procedure checklists, recovery timeline with Dos & Don'ts, success rates, risks and complications, fertility outcomes, and how embolization compares to surgery — so you can make a fully informed decision before your consultation.
QUICK ANSWER:
Varicocele Embolization in Hyderabad — Key Facts
Non-surgical | 85–90% Success | 15-45 Min | Same-Day Discharge | 1-2 Day Recovery | No Incision | No Stitches
Book Varicocele Embolization Consultation — Citi Vascular Hospital, Kukatpally, Hyderabad
+91-73375 83901 | WhatsApp | citivascularcentre.com
No Surgery | Same-Day Discharge | 85–90% Success | Insurance Assisted | Dr. Garge FRCR (UK)
|
Feature |
Details |
|
Procedure Type |
Minimally Invasive Interventional Radiology — image-guided, no open surgery |
|
Anaesthesia |
Local anaesthesia + conscious sedation — no general anaesthesia |
|
Incision Required? |
❌ No — 2mm neck or groin puncture only |
|
Stitches Required? |
❌ No — puncture seals naturally |
|
Procedure Duration |
15-45 minutes (unilateral); 30–60 minutes (bilateral) |
|
Hospital Stay |
Same-day discharge — day-care procedure |
|
Return to Work |
1-2 days (desk work); 5–7 days (physical work) |
|
Technical Success Rate |
85–90% symptom relief (pain + semen parameter improvement) |
|
Recurrence Rate |
~5–10% |
|
Fertility Improvement |
Possible in 60–70% of infertility-related varicocele cases |
|
Bilateral Treatment |
✅ Both sides treated simultaneously — single session |
|
Access Route |
neck (jugular) or groin (femoral) vein — surgeon's preference |
|
Specialist Required |
Interventional Radiologist — not a urologist or general surgeon |
|
Available At |
Citi Vascular Hospital, Kukatpally Colony, Road No. 1, Hyderabad — Dr. Shaileshkumar Garge FRCR (UK) |
Definition:
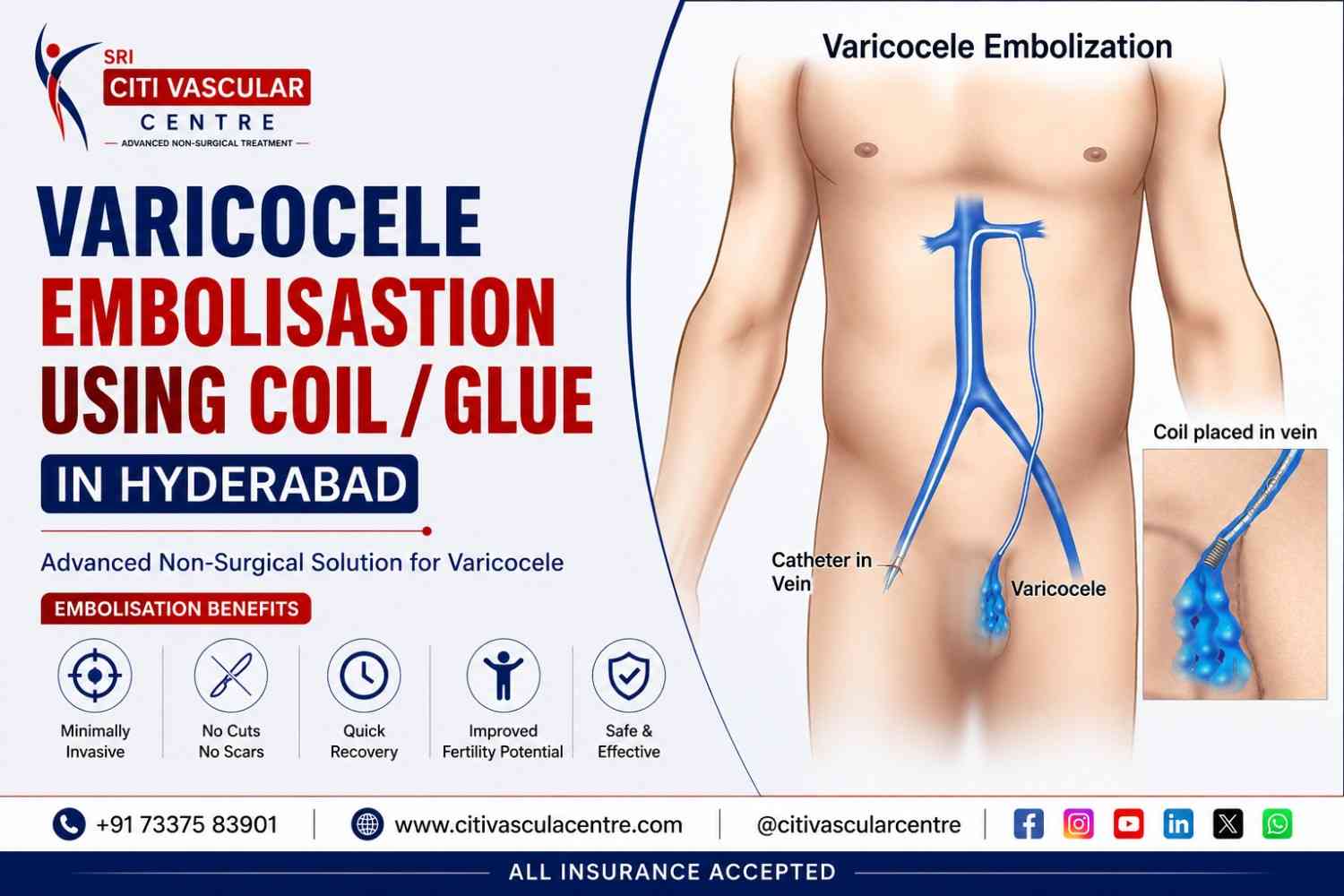
Varicocele embolization is a non-surgical, image-guided procedure performed by an Interventional Radiologist to permanently block the abnormal veins (pampiniform plexus) responsible for varicocele — enlarged veins within the scrotum that can cause pain, testicular atrophy, and male infertility.
Unlike varicocelectomy (surgical ligation), embolization does not require any surgical incision in the scrotum, groin, or abdomen. Instead, a tiny 2mm catheter is guided through a vein in the neck or groin under live real-time X-ray (fluoroscopy) to the internal spermatic vein, where embolic agents are delivered to block abnormal blood flow.
Who Performs Varicocele Embolization?
Varicocele embolization is exclusively performed by Interventional Radiologists — specialists trained in image-guided minimally invasive vascular procedures. It is NOT performed by urologists, general surgeons, or andrologists. Dr. Shaileshkumar Garge at Citi Vascular Hospital, Kukatpally, Hyderabad holds FRCR (UK), FNVIR (CMC Vellore), Fellowship (USA) and EBIR (Spain) — triple international credentials in interventional radiology.
Varicocele Embolization vs Varicocelectomy — One-Line Difference
Varicocele embolization = blocking abnormal veins from the inside through a vein in the neck or groin, using a tiny catheter under fluoro guidance — no surgical cuts, no stitches, local anaesthesia only.Varicocelectomy = surgically cutting and tying the abnormal veins through an incision in the groin, abdomen, or scrotum — general/spinal anaesthesia, stitches, 5–14 day recovery.
Mechanism of Varicocele Formation — Stage Table
|
Stage |
Phase |
What Happens |
Clinical Impact |
|
1 |
Normal Anatomy |
Venous valves in the internal spermatic vein prevent blood from flowing backwards |
Normal venous drainage — no varicocele |
|
2 |
Valve Dysfunction |
Venous valves become incompetent — blood flows backwards (reflux) toward the testicle |
Pressure builds in the pampiniform plexus |
|
3 |
Venous Dilatation |
Pampiniform plexus veins dilate > 3mm due to increased backflow pressure |
Clinically palpable varicocele — 'bag of worms' sensation |
|
4 |
Thermal Effect |
Pooled blood raises scrotal temperature by 1–2°C above normal testicular temperature |
Spermatogenesis impaired — sperm count and motility decline |
|
5 |
Progressive Damage |
Prolonged elevated pressure and temperature may cause testicular atrophy over time |
Testicular volume decreases — function deteriorates if untreated |
|
6 |
Embolization Reverses This |
Embolic agents permanently block the incompetent internal spermatic vein — blood rerouted to healthy collaterals |
Venous pressure drops | temperature normalises | symptoms improve |
Key Clinical Insight: Varicocele embolization works by permanently eliminating the root cause — incompetent venous reflux in the internal spermatic vein. It does not simply 'treat symptoms' — it physiologically corrects the abnormal blood flow that causes the scrotal venous congestion
Candidacy Table — Is Embolization Right for You?
|
Clinical Situation |
Embolization Suitable? |
Clinical Rationale |
|
Persistent scrotal pain/discomfort > 3 months |
✅ Yes |
Pain from venous congestion — embolization removes the backflow pressure causing it |
|
Male infertility with varicocele on Doppler |
✅ Yes |
85–90% technical success; 60–70% semen parameter improvement in 3–6 months |
|
Bilateral varicocele (left + right) |
✅ Preferred |
Both sides treated simultaneously in ONE session — not possible with surgery without two procedures |
|
Recurrent varicocele after prior surgery |
✅ Strongly preferred |
Avoids re-dissection of scarred tissue from prior operation — technically simpler than repeat surgery |
|
Testicular atrophy / size discrepancy |
✅ Urgent referral |
Untreated varicocele may progressively reduce testicular volume and long-term function |
|
Wishes to avoid general anaesthesia |
✅ Yes |
Local anaesthesia only — suitable for men with anaesthesia concerns or co-morbidities |
|
Abnormal semen analysis confirmed |
✅ Yes |
Semen parameters (count, motility, morphology) may improve significantly post-embolization |
|
Small subclinical varicocele — no symptoms |
⚠️ Discuss |
Treatment may not be required — watchful waiting and annual Doppler follow-up appropriate |
Contraindications: Varicocele embolization is NOT suitable for: men with severe contrast allergy (relative — may be manageable), severely impaired renal function (contrast risk), active pelvic infection, or known venous anomalies requiring surgical management. All of these are assessed at the pre-procedure consultation with Dr. Garge at Citi Vascular, Kukatpally.
Access Route — Neck vs Groin
|
Feature |
jugular Access (neck) |
Femoral Access (Groin) |
|
Entry Point |
Jugular vein at neck |
Femoral vein at groin |
|
Patient Comfort |
Higher — neck easier to hold still; patient can move freely |
Lower — patient must keep leg still; firm pressure post-procedure |
|
Post-Procedure |
neck band applied — can sit and walk immediately |
Firm compression 15–20 min — limited mobility briefly |
|
Scar / Mark |
Tiny 1–2mm mark at neck — nearly invisible |
Small mark at groin — fades quickly |
|
Preferred At Citi Vascular |
Used when femoral approach not feasible |
Femoral (groin) approach preferred when anatomically suitable |
Embolic Materials — Types and Clinical Use
|
Material Type |
How It Works |
Best Used For |
Key Advantage |
|
Coils (Platinum/Steel) |
Mechanical plug — coils expand to fill and block the vein lumen permanently |
Primary embolization of internal spermatic vein |
Permanent, precise, immediately effective. Industry gold standard. |
|
Sclerosant Foam (Polidocanol / STS) |
Chemical agent injected into vein lining — causes inflammatory closure over days |
Small collateral branches; combined with coils for complete occlusion |
Treats small residual branches that coils cannot reach |
|
Liquid Embolic Agents - Glue |
Viscous polymer that solidifies on contact with blood — fills complex venous anatomy |
Complex or recurrent varicocele anatomy; tortuous veins |
Excellent for recurrent cases where anatomy is variable post-surgery |
|
Combined Technique |
Coils proximally + sclerosant distally — ensures no residual patent branches |
Bilateral varicocele; complex anatomy; infertility cases where complete occlusion essential |
Lowest recurrence rate — most comprehensive blockade of abnormal venous network |
Dr. Garge at Citi Vascular Hospital, Kukatpally, selects embolic material based on: venous anatomy on Doppler/venography, unilateral vs bilateral disease, prior surgery history, and whether fertility optimisation is the primary goal. All techniques are available in-house — no referral needed.
Technical Approaches — Antegrade vs Retrograde
|
Approach |
Retrograde Embolization |
Antegrade Embolization |
|
Entry |
Via jugular vein (neck) or femoral vein (groin) — catheter advanced DOWN into spermatic vein from above |
Direct puncture of the spermatic vein in the groin — catheter advanced into varicose veins from below |
|
Standard Use |
✅ Standard technique for primary varicocele embolization worldwide |
Used for recurrent cases or when retrograde access is anatomically difficult |
|
Advantages |
Accurate catheter placement under fluoroscopy; good visualisation of entire venous system |
Direct access to target veins; useful in post-surgical anatomy |
|
Used At Citi Vascular |
Primary technique for most cases |
Selected for recurrent varicocele post-surge |
Complete Pre-Procedure Checklist — What to Do Before Varicocele Embolization
|
When |
Preparation Step |
Details / Notes |
|
2–4 Weeks Before |
Scrotal Doppler Ultrasound |
Confirms varicocele grade, vein diameter, reflux, and bilateral involvement — essential for embolization planning |
|
2–4 Weeks Before |
Semen Analysis (if infertility concern) |
Establishes baseline sperm count, motility, and morphology to measure improvement at 3-month follow-up |
|
1–2 Weeks Before |
Pre-Procedure Consultation with Dr. Garge |
Medical history review, medication assessment, technique discussion, insurance pre-authorisation initiated |
|
1 Week Before |
Medication Review |
Blood-thinning medications (aspirin, warfarin, clopidogrel, NSAIDs) reviewed — paused if medically appropriate per Dr. Garge's advice |
|
1 Week Before |
Blood Tests |
Full blood count, renal function (for contrast safety), coagulation profile, blood group — all pre-procedure safety screening |
|
Day Before |
Fasting Instructions |
Light meal up to 6 hours before procedure. Clear fluids up to 2 hours before. Follow specific instructions from Citi Vascular team. |
|
Day Before |
Hydration |
Drink adequate water — good hydration reduces contrast-related kidney stress. No alcohol 24 hours before. |
|
Day of Procedure |
Clothing + Hygiene |
Shower morning of procedure. Wear loose, comfortable clothing. No jewellery on neck if jugular access planned. |
|
Day of Procedure |
Arrange Transportation |
Cannot drive yourself home — arrange a companion or taxi. You may feel mildly drowsy from sedation. |
|
Day of Procedure |
Bring Documents |
ID, insurance card, referral letter, all prior scan reports (Doppler USG, semen analysis), blood test results |
|
At Registration |
Final Consent |
Dr. Garge explains the procedure, access route, embolic materials to be used, and answers final questions. Written consent obtained. |
Insurance Pre-Authorisation: If your treatment is covered by corporate mediclaim, CGHS, or other schemes, pre-authorisation paperwork is completed 1–2 weeks before the procedure. Citi Vascular Hospital, Kukatpally, handles all documentation on your behalf. Call +91-73375 83901 early to allow time for this process.
Complete 8-Step Procedure Guide
|
1 |
Arrival, Assessment & Consent You arrive at Citi Vascular Hospital, Kukatpally, 1–2 hours before the procedure. Registration is completed. Vital signs (blood pressure, heart rate, temperature) are checked. Previous imaging and blood test results are reviewed by Dr. Garge. Any remaining questions are answered. Written informed consent is signed confirming understanding of the procedure, risks, and alternatives. |
|
2 |
Pre-Procedure Setup & IV Access An IV cannula is placed in the arm for medication administration. Light pre-procedural sedation or analgesia may be given to ensure comfort. You are positioned on the fluoroscopy table. The access site — neck (jugular) or groin (femoral) — is cleaned, sterilised, and draped. Local anaesthetic cream may be applied 2-5 minutes before injection. |
|
3 |
Local Anaesthesia Injection — neck or Groin A small amount of local anaesthetic (lignocaine) is injected precisely at the access site. You feel a brief sharp sting for 5–10 seconds — after which the area becomes completely numb. This is typically the most uncomfortable moment of the entire procedure. Dr. Garge ensures adequate numbness before proceeding with catheter insertion. |
|
4 |
Catheter Insertion & Navigation A 4–5 French sheath (thin tube, ~2mm diameter) is inserted through the numbed puncture site into the vein. A flexible catheter-guide wire is advanced under live fluoroscopy guidance through the venous system to the left internal spermatic vein — the primary vein responsible for left-sided varicocele. For right-sided or bilateral varicocele, the catheter is repositioned to access the right gonadal vein. |
|
5 |
Venography — Mapping the Abnormal Veins A small volume of contrast dye is injected through the catheter directly into the internal spermatic vein. Under fluoroscopy, this creates a roadmap of the entire abnormal venous network — showing which branches are dilated, where reflux occurs, and identifying collateral veins that must also be blocked. This critical mapping step takes 3–6 minutes and determines which embolic materials and quantities are needed. |
|
6 |
Embolization — Permanent Blockade of Abnormal Veins Embolic agents are precisely delivered through the catheter into the abnormal internal spermatic vein and its branches. Platinum coils are deployed first to mechanically block the main vessel. If sclerosant foam or liquid embolic is also planned (combined technique), this is delivered after coil placement to treat smaller collateral branches. Repeat fluoroscopy images confirm complete occlusion — no residual flow visible. |
|
7 |
Bilateral Treatment (If Applicable) If bilateral varicocele is present, the catheter is repositioned to the right gonadal vein through the same access point or a second puncture. The venography and embolization steps (Steps 5–6) are repeated for the right side. Treating both sides in a single session is one of embolization's key advantages over surgery, which would require two separate procedures. |
|
8 |
Final Verification Imaging, Sheath Removal & Recovery A final fluoroscopy run confirms complete embolization — no contrast flow in the treated veins. The catheter and sheath are removed. At the neck: a compression neckband is applied for 2–3 hours. At the groin: firm manual pressure for 10–15 minutes followed by a pressure dressing. You are moved to the recovery bay for 1–2 hours of monitoring. Vital signs are checked. Mild pelvic or flank discomfort is normal and managed with oral pain medication. Same-day discharge in most cases. |
Total Procedure Time: Unilateral varicocele embolization takes approximately 15–45 minutes. Bilateral (both sides) takes 30–60 minutes. Combined technique with additional sclerosant may add 10–15 minutes. The total clinic time from arrival to discharge is approximately 3–4 hours.
Intra-Procedure Patient Journey — What You Experience
|
Phase |
Sensation / Experience |
What the Doctor Is Doing |
|
Local anaesthetic |
Brief sharp sting for 5–10 sec then numbness |
Injecting lignocaine precisely at access site |
|
Catheter insertion |
Pressure sensation — no pain |
Advancing sheath through neck or groin vein |
|
Navigation |
No sensation at all — veins have no pain receptors |
Guiding wire + catheter under fluoroscopy to spermatic vein |
|
Venography |
Mild warmth/flush in pelvis when contrast injected — normal |
Injecting contrast to map abnormal venous anatomy |
|
Embolization |
Mild dull ache or pelvic heaviness — managed with pain meds |
Deploying coils/foam to block internal spermatic vein |
|
Completion |
Relief — procedure feels finished |
Final imaging to confirm complete blockade |
|
Post-procedure |
Mild soreness — well-managed orally |
Monitoring vitals | applying dressing | completing discharge |
|
Timeframe |
What to Expect |
Dos & Don'ts |
|
Day 0 — Procedure Day |
Mild pelvic/flank ache as local anaesthetic wears off. Possible mild nausea from sedation. The neck or groin site is tender. |
✅ Rest at home. ✅ Oral pain meds. ❌ No driving same day. ❌ No heavy lifting. |
|
Days 1–2 |
Dull pelvic heaviness improving gradually. Minor bruising at access site normal. Mild fatigue expected. |
✅ Gentle walking. ✅ Paracetamol/ibuprofen. ❌ No gym. ❌ No cycling. ❌ No sex. |
|
Days 2–3 |
Most men feel significantly better. Light daily activities resume. Appetite returns to normal. |
✅ Desk work. ✅ Short drives. ✅ Light cooking. ❌ No strenuous activity. |
|
Days 5–7 |
Return to full daily activities for most patients. Access site healed. Scrotal heaviness reducing. |
✅ Full normal routine. ✅ Sexual activity after Day 7. ❌ No heavy physical labour yet. |
|
Week 2 |
Full return to physical activity including exercise, gym, and cycling for most patients. |
✅ Full exercise. ✅ All activities. Report any fever > 38°C or worsening pain. |
|
Month 1–3 |
Progressive reduction in scrotal vein congestion as embolized veins are reabsorbed. Pain steadily improves. |
✅ Follow-up Doppler at 3 months to confirm successful occlusion of treated veins. |
|
Month 3–6 |
Semen analysis at 3–6 months to assess sperm parameter improvement. Most fertility benefits are seen by 6 months. |
✅ Semen analysis. ✅ Consult fertility specialist if pregnancy not achieved by 6 months. |
Post-Embolization Syndrome: Some patients experience mild fever (up to 38°C), pelvic ache, and fatigue for 2–4 days after varicocele embolization. This is a normal inflammatory response to the embolized vein tissue — NOT infection. It resolves with rest, paracetamol, and adequate fluids. Contact Dr. Garge at Citi Vascular Kukatpally if fever exceeds 38.5°C or does not resolve by Day 5.
|
Clinical Outcome |
Success Rate / Data |
Source / Context |
|
Technical success (vein occlusion confirmed) |
95–98% |
Venography confirms blocked vein on same-day imaging |
|
Overall symptom relief (pain + quality of life) |
85–90% |
Prospective cohort studies; CIRSE / SIR data |
|
Scrotal pain improvement |
75–90% |
Pain resolves/reduces within 4–12 weeks in most cases |
|
Semen parameter improvement (count/motility) |
60–70% of infertility cases |
3–6 month post-procedure semen analysis |
|
Spontaneous pregnancy rate post-embolization |
Variable — 30–45% |
Depends on female fertility, varicocele grade, and baseline semen |
|
Testicular volume preservation |
Maintained in most cases |
Atrophy progression halted after successful embolization |
|
Recurrence rate |
~5–10% at 2 years |
Lower with combined coil + sclerosant technique |
|
Hydrocele formation (vs surgery) |
< 1% |
Major advantage over surgery where hydrocele risk is 5–10% |
|
Patient satisfaction |
85–90% |
Published patient-reported outcome surveys |
Important: Varicocele embolization improves the conditions for better sperm production — it does not directly produce sperm. Semen parameter improvement typically takes 3–6 months as the sperm production cycle (spermatogenesis) takes ~74 days. Patients should not expect immediate fertility improvement and should follow up with a semen analysis at 3 and 6 months.
|
Risk Category |
Specific Risk |
Frequency |
Management |
|
Very Common (>20%) |
Mild pelvic/flank ache post-procedure |
Almost all patients |
Oral paracetamol/ibuprofen — resolves in 1–3 days |
|
Common (5–20%) |
Access site bruising/soreness (neck or groin) |
~20–30% |
Self-resolving in 5–10 days with ice + rest |
|
Uncommon (1–5%) |
Post-embolization syndrome (fever, fatigue, ache) |
~10–20% |
Normal inflammatory response — paracetamol + fluids + rest |
|
Uncommon (1–5%) |
Pampiniform plexus phlebitis (vein inflammation) |
~3–5% |
NSAIDs + scrotal support — self-resolving in 1–2 weeks |
|
Rare (< 1%) |
Coil migration to pulmonary vasculature |
< 0.5% |
Occurs only with undersized coils — expert technique prevents this |
|
Rare (< 1%) |
Pelvic or testicular infection |
< 1% |
Antibiotic course — sterile technique reduces risk |
|
Rare (< 1%) |
Contrast allergy / renal reaction |
< 0.5% |
Pre-screened + pre-medicated — managed in Cath Lab |
|
Procedural (~5–10%) |
Varicocele recurrence |
~5–10% at 2 years |
Repeat embolization or surgical ligation if symptomatic |
Contact Citi Vascular Hospital Immediately (+91-73375 83901) If: Fever > 38.5°C not improving after Day 3 | Increasing (not decreasing) scrotal or pelvic pain after Day 3 | Worsening significant swelling at access site | Feeling systemically very unwell (chills, rigors, nausea). Most varicocele embolizations are uncomplicated — these symptoms are rare but require prompt review.
How Embolization May Improve Fertility — Mechanism
|
What Changes After Embolization |
How This Improves Fertility |
|
Venous reflux permanently blocked |
Backflow of blood from renal / adrenal veins into spermatic vein stops — primary cause of damage eliminated |
|
Scrotal temperature normalises |
Elevated scrotal temperature (1–2°C above ideal) returns to normal — spermatogenesis resumes optimally |
|
Testicular oxidative stress reduces |
Reduction in reactive oxygen species in the scrotal environment — less DNA fragmentation in sperm |
|
Hormone levels may improve |
LH and FSH levels may normalise — Leydig cell testosterone production can improve in selected cases |
|
Venous congestion resolves |
Reduced venous pooling lowers intratesticular pressure — blood flow improves | nutrient delivery to seminiferous tubules increases |
⏳ Fertility Timeline After Embolization: The human spermatogenesis cycle takes approximately 74 days. Do NOT expect semen improvement in the first 3 months. First semen analysis should be done at 3 months, with the definitive assessment at 6 months. Most fertility improvement, if it occurs, is measurable by 6 months post-embolization.
Fertility FAQ Table — Most-Searched Fertility Questions
|
Patient Question |
Clinical Answer |
|
Does embolization always improve fertility? |
No. ~60–70% of men see semen parameter improvement. Spontaneous pregnancy rates vary: ~30–45%, depending heavily on female partner fertility, baseline sperm parameters, and duration of infertility. |
|
Is embolization as good as microsurgery for fertility? |
Studies show comparable outcomes for both techniques. Microsurgery may have marginally lower recurrence rate. Embolization has lower hydrocele risk. Fertility outcomes are broadly similar. Dr. Garge advises individually based on anatomy and clinical factors. |
|
When should I have a semen analysis after embolization? |
At 3 months and again at 6 months post-embolization. This covers 2 full spermatogenesis cycles. If significant improvement in parameters is not seen by 6 months, reassessment with a fertility specialist is recommended. |
|
Can embolization be done if we're doing IVF/ICSI? |
Yes. Embolization is often recommended even before IVF/ICSI to improve sperm quality — better sperm = better IVF outcomes. The procedure can be timed 3–6 months before the planned IVF cycle for maximum benefit. |
|
Feature |
Embolization |
Microsurgery |
Laparoscopic |
Open Surgery |
|
Surgical Incision |
❌ None |
✅ Inguinal |
✅ Abdominal |
✅ Scrotal/Inguinal |
|
Stitches |
❌ None |
✅ Yes |
✅ Yes |
✅ Yes |
|
Anaesthesia |
Local only |
General/Spinal |
General |
General/Spinal |
|
Duration |
15-45 min |
45–90 min |
45–75 min |
45–60 min |
|
Hospital Stay |
Same day |
1–2 days |
1–2 days |
1-2 day |
|
Return to Work |
1-2 days |
7–10 days |
7–10 days |
7–14 days |
|
Hydrocele Risk |
< 1% |
~2–5% |
~5–10% |
~10–15% |
|
Recurrence Rate |
~5–10% |
~1–5% |
~3–7% |
~10–15% |
|
Bilateral Same Session? |
✅ Yes |
2 procedures |
Usually yes |
2 procedures |
|
Success Rate |
85–90% |
75–90% |
70–85% |
70–80% |
|
Ideal For |
Pain, infertility, bilateral, recurrent |
Infertility, lowest recurrence |
General surgical approach |
Limited anatomy for microsurgery |
For Recurrent Varicocele After Surgery: Embolization is the PREFERRED treatment. Repeat surgery through scarred tissue is technically very difficult and carries higher complication risk. Embolization avoids the prior surgical site entirely — approaching the abnormal veins from the neck or groin through a completely fresh pathway.
|
Treatment |
Approximate All-Inclusive Cost — Citi Vascular Kukatpally, Hyderabad 2026 |
|
Varicocele Embolization (Unilateral) |
₹60,000–₹1,40,000 all-inclusive |
|
Varicocele Embolization (Bilateral — Both Sides) |
₹90,000–₹2,20,000 all-inclusive |
|
Open Varicocelectomy |
₹40,000–₹80,000 |
|
Microsurgical Varicocelectomy |
₹70,000–₹1,50,000 |
Insurance assistance, EMI payment options, and cashless facility are available at Citi Vascular Hospital, Kukatpally, Hyderabad. For a complete cost breakdown including component-wise pricing, insurance coverage table, EMI amounts, and total economic cost comparison — see our dedicated guide:
Full Cost Guide: Varicocele Treatment Cost in Hyderabad 2026 — citivascularcentre.com/varicocele-treatment-cost-in-hyderabad Covers: component breakdown | bilateral vs unilateral pricing | insurance types + documentation | EMI monthly amounts | total economic cost vs surgery
Sudhir's Story — 29-Year-Old Software Engineer, Hitech City, Hyderabad
|
Stage |
Arjun's Experience |
Clinical Details |
|
Presentation |
Left-sided scrotal heaviness + ache for 8 months | Couple trying to conceive for 1 year |
Classic symptomatic varicocele presentation with concurrent infertility concern |
|
Diagnosis |
Scrotal Doppler at Citi Vascular confirmed left Grade 3 varicocele with reflux | Semen analysis: low motility |
Doppler — vein diameter 3.8mm, confirmed reflux on Valsalva | Baseline semen established |
|
Consultation |
Dr. Garge explained embolization vs microsurgery | Both options discussed openly | Joint decision with wife |
Bilateral assessment confirmed — left-sided only | Embolization recommended as first-line option |
|
Procedure Day |
Arrived 9 AM | Procedure at 10:30 AM | Left at 1 PM |
30-minute procedure | femoral access | Coil + foam combined technique | Same-day discharge |
|
Recovery |
Day 1–2: mild ache managed with ibuprofen | Day 3: back to desk work | Day 7: full activity |
No complications | Access site healed | Follow-up Doppler booked at 3 months |
|
3-Month Review |
Doppler: successful occlusion confirmed | Semen motility improved significantly |
Semen count and motility both improved at 3-month analysis | Continued monitoring |
"The procedure was nothing like what I feared. I was awake the entire time — felt only mild pressure. Home the same afternoon. My wife and I came together for the consultation — Dr. Garge answered all our questions clearly. At the 3-month scan, the embolization had worked exactly as described." — Sudhir, 29, Hitech City
|
Credential |
Detail |
|
Full Name |
Dr. Shaileshkumar Garge |
|
Qualifications |
MBBS | MD (Mumbai) | DNB (Delhi) | FRCR (UK) | FNVIR (CMC Vellore) | EBIR (Spain/Europe) | Fellowship (North Carolina, USA) |
|
Role |
Director & Chief Vascular Physician | Senior Consultant Interventional Radiologist |
|
Hospital |
Citi Vascular Hospital, Kukatpally Colony, Road No. 1, Hyderabad, Telangana 500072 |
|
Varicocele Specialisation |
Non-surgical varicocele embolization | bilateral treatment | recurrent varicocele after surgery | infertility-related embolization |
|
Experience |
12+ years | 15,000+ minimally invasive vascular procedures |
|
Technology |
Dedicated Cath Lab | Real-time Fluoroscopy | Colour Doppler Ultrasound | Advanced Embolic Materials |
|
Other Specialisations |
Embolisation, UFE/UAE, Varicose Veins, PAD, DVT, Pelvic Congestion Syndrome, Vascular Malformations |
|
Serving |
Kukatpally, KPHB, Miyapur, Hitech City, Ameerpet, Secunderabad, Hyderabad & Telangana |
Q1: Is varicocele embolization painful?
Varicocele embolization is performed under local anaesthesia with conscious sedation — so you are awake but comfortable throughout. The only discomfort is a brief sting during the local anaesthetic injection (5–10 seconds). During the procedure itself, you feel pressure but no pain. Afterward, mild pelvic or flank ache for 1–3 days is normal and is effectively managed with oral pain medication.
Q2: How long does varicocele embolization take?
Unilateral varicocele embolization (one side) takes approximately 15–45 minutes. Bilateral embolization (both sides treated in one session) takes 30–60 minutes. Combined coil + sclerosant technique adds 10–15 minutes. Total clinic time from arrival to discharge is approximately 3–4 hours, including pre-procedure assessment and 1–2 hours of post-procedure recovery monitoring at Citi Vascular Hospital, Kukatpally, Hyderabad.
Q3: Is hospitalisation required for varicocele embolization?
No. Varicocele embolization is a day-care procedure — you arrive, have the procedure, rest in the recovery bay for 1–2 hours, and go home the same day. No overnight hospital admission is required. This is one of the key advantages over surgical varicocelectomy, which typically requires 1–2 nights in hospital. Most patients are discharged within 3–4 hours of arrival at Citi Vascular Hospital, Kukatpally.
Q4: When can I return to work after varicocele embolization?
Most men return to desk work and light activities within 1-2 days after varicocele embolization. Physical jobs involving heavy lifting, construction, or strenuous activity require 5–7 days of rest. Full exercise including gym and cycling can resume by Day 7–10. This is significantly faster than recovery from varicocele surgery, which typically requires 7–14 days off work for most techniques.
Q5: Does varicocele embolization improve fertility and sperm count?
Varicocele embolization improves semen parameters in approximately 60–70% of infertility-related cases — including sperm count, motility, and morphology. Semen improvement takes 3–6 months as the spermatogenesis cycle requires ~74 days. A semen analysis at 3 months and 6 months post-procedure monitors progress. Spontaneous pregnancy rates after embolization are approximately 30–45%, depending on female partner fertility and baseline semen quality.
Q6: What types of embolic materials are used in varicocele embolization?
Varicocele embolization uses three main embolic materials: (1) Platinum coils — permanent mechanical plugs that block the main internal spermatic vein, (2) Sclerosant foam (polidocanol or sodium tetradecyl sulfate) — chemical agents that close smaller collateral branches, and (3) Liquid embolics Glue — for complex or recurrent anatomy. Dr. Garge at Citi Vascular Kukatpally selects the technique based on venography findings.
Q7: Can bilateral varicocele be treated in one session?
Yes — one of varicocele embolization's most significant advantages. Both left and right varicoceles are treated in a single 30–60 minute session through the same neck or groin access point. Surgical varicocelectomy requires two separate operations for bilateral disease — meaning two separate hospital admissions, two separate recoveries, and approximately double the surgical risk. At Citi Vascular Kukatpally, bilateral embolization is performed routinely.
Q8: What is the success rate of varicocele embolization?
Varicocele embolization achieves: 95–98% technical success (confirmed vein occlusion on same-day imaging), 85–90% overall symptom relief (pain improvement + quality of life), 60–70% semen parameter improvement in infertility-related cases, and approximately 5–10% recurrence rate at 2 years. Combined coil + sclerosant technique achieves the lowest recurrence rates. These outcomes are comparable to microsurgical varicocelectomy without requiring general anaesthesia.
Q9: Can recurrent varicocele after surgery be treated by embolization?
Yes — and embolization is the preferred treatment for recurrent varicocele following prior surgery. Repeat surgical dissection through scarred tissue from the previous operation is technically difficult and carries higher complication risk. Embolization approaches the abnormal internal spermatic vein from the neck or groin — avoiding the prior surgical site entirely. Dr. Garge at Citi Vascular, Kukatpally, has specific experience in recurrent varicocele embolization.
Q10: What is the cost of varicocele embolization in Hyderabad?
Varicocele embolization costs approximately ₹60,000–₹1,40,000 all-inclusive at Citi Vascular Hospital, Kukatpally, Hyderabad in 2026. Bilateral embolization (both sides) is ₹90,000–₹2,20,000. All-inclusive means: consultation, Doppler imaging, procedure, embolic materials, anaesthesia, medications, and follow-up. Insurance is often available. For a full cost breakdown with EMI options, see: citivascularcentre.com/varicocele-treatment-cost-in-hyderaba
Citi Vascular Hospital, Kukatpally Colony, Road No. 1, Hyderabad is easily accessible for varicocele embolization consultations from:
Kukatpally & KPHB — 5 min drive via Kukatpally Main Road
Miyapur & Bachupally — 10 min via Miyapur X Roads
Hitech City & Madhapur — 20 min via IT Corridor
Ameerpet & SR Nagar — 20 min via Balanagar flyover
Gachibowli & Kondapur — 25 min via PVNR Expressway
Secunderabad & Begumpet — 25 min via NH 65
Kompally, Medchal & Alwal — 20–25 min via ORR
|
Hospital |
Contact |
Location & Hours |
|
Citi Vascular Hospital |
+91-73375 83901 |
Kukatpally Colony, Road No. 1, Hyderabad, Telangana 500072 | Mon–Sat 9AM–6PM |
|
Book Consultation |
citivascularcentre.com |
WhatsApp + Online booking | Same-day consultation available | Free parking |
|
✅ |
Non-surgical — no incision, no stitches, no general anaesthesia required |
|
✅ |
95–98% technical success confirmed on same-day fluoroscopy imaging |
|
✅ |
85–90% overall symptom relief — pain, heaviness, quality of life |
|
✅ |
60–70% semen parameter improvement in infertility-related varicocele |
|
✅ |
Bilateral treatment in ONE session — left + right varicocele |
|
✅ |
Same-day discharge — return to desk work within 1-2 days |
|
✅ |
Preferred for recurrent varicocele after prior surgery |
|
✅ |
< 1% hydrocele risk — major advantage over surgery (5–15%) |
|
✅ |
Performed by Dr. Shaileshkumar Garge FRCR (UK), EBIR (Spain), Fellowship (USA) — 12+ years, 15,000+ procedures |
|
✅ |
Insurance assisted | EMI available | Transparent all-inclusive pricing from ₹60,000 |
Varicocele embolization in Hyderabad at Citi Vascular Hospital, Kukatpally, is an advanced non-surgical treatment that permanently blocks the abnormal internal spermatic vein through a 2mm neck or groin puncture — no incision, no stitches, local anaesthesia only. With 85–90% clinical success, same-day discharge, 2–3 day recovery, bilateral treatment in one session, and significant fertility benefits in appropriately selected men, it is the preferred treatment for most symptomatic varicoceles in 2026.
If you have scrotal pain, abnormal semen parameters, testicular size discrepancy, or a varicocele on Doppler ultrasound — an expert consultation with Dr. Shaileshkumar Garge, FRCR (UK), at Citi Vascular Hospital, Kukatpally, Hyderabad will determine whether varicocele embolization is the right t